Orthopedic surgery is one of the most modifier-intensive specialties in healthcare — and those modifiers directly determine reimbursement.
They are not administrative details. They are payment drivers.
A missing RT modifier. An incorrect 50 modifier. Improperly reporting an assistant surgeon instead of a co-surgeon.
Each of these can mean the difference between full reimbursement and reduced payment — or worse, an automatic denial.
Too often, billing vendors treat modifiers as coding add-ons instead of revenue levers. But in orthopedics, small modifier mistakes create large financial consequences. And when combined with enrollment or payer policy issues, those errors compound quickly: a risk also discussed in:
👉 Medical Credentialing Services: The Revenue Risk Most Practices Overlook.
Orthopedic groups cannot afford to treat modifier accuracy as optional.
Why Orthopedic Modifiers Are More Complex Than Other Specialties
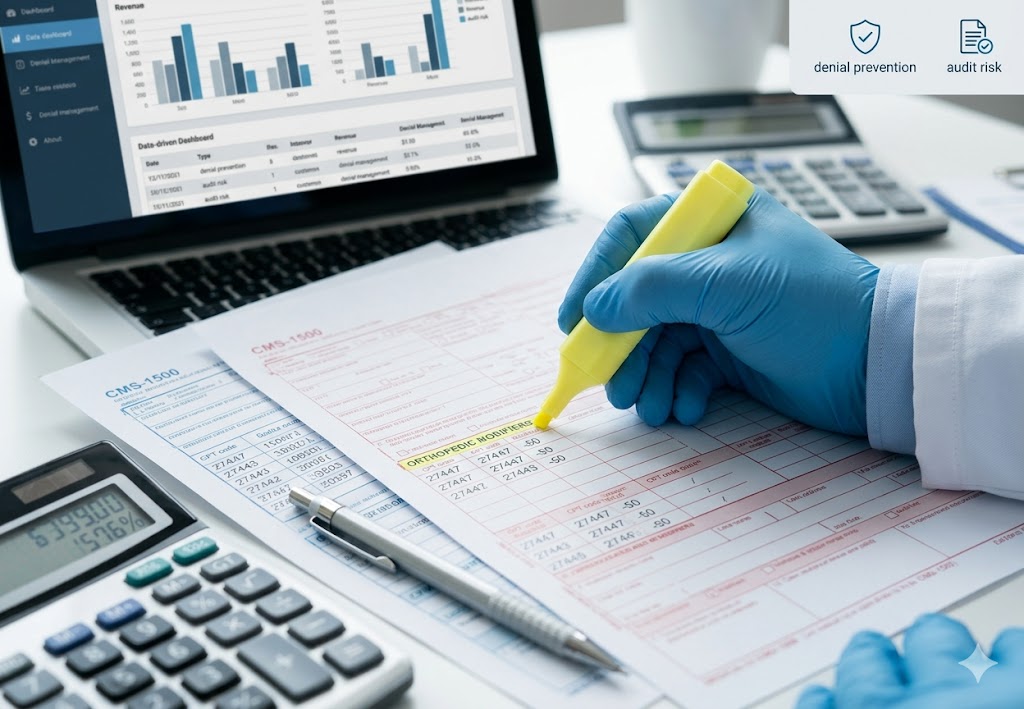
Orthopedics involves high-complexity procedures, bilateral surgeries, multi-physician participation, imaging, and injectable therapies — all of which require precise modifier reporting.
Anatomical Modifiers (RT, LT, and Bilateral Distinctions)
Orthopedic claims frequently require anatomical modifiers such as RT (Right side), LT (Left side), and specific digits of fingers (FA-F9) and toes (TA`-T9). Without these, claims often fail payer edits for insufficient specificity. Moreover, when an ICD-10 provides specificity for the anatomical site, the informational modifiers must be in consistent alignment.
Bilateral procedures introduce additional complexity. Incorrect use of modifier 50 can lead to underpayment, duplicate denials, or reimbursement reductions. While Medicare has established guidelines for Modifier 50, private payers often maintain unique policies. For instance, some require separate line items for bilateral procedures (using RT/LT modifiers and a 59 modifier on the second line) rather than a single bilateral modifier. Over time, it is these small discrepancies that accumulate into larger losses — exactly the type of margin erosion discussed in 👉Are Underpayments Eroding Your Practice’s Margins?
In high-volume orthopedic practices, even minor bilateral reporting errors can translate into thousands in lost revenue if the practitioner is only paid for half of the rendered services.
Surgical Role Modifiers and Reimbursement Implications
Orthopedic procedures often involve assistant surgeons, co-surgeons, or surgical teams. Each role requires a specific modifier, and each payer reimburses those roles at a different percentage of the full physician fee schedule.
Improper designation can result in:
- Reduced reimbursement percentages
- Automatic denials
- Requests for operative documentation
Specialty billing complexity is not unique to orthopedics. As explored in 👉The Anesthesia Revenue Gap: Why Clinical Excellence Doesn’t Guarantee Financial Health, specialty-specific reimbursement nuances frequently create hidden revenue gaps when billing is not aligned with payer expectations.
Orthopedic modifier errors produce similar financial exposure.
Technical vs. Professional Component Modifiers in Imaging
Orthopedic practices commonly perform imaging services within the office to provide more timely, effective care to patients. We see payers that attempt to pay for only the professional interpretation (26) or technical component (TC), rather than the complete global service that the orthopedic surgeon is due when the clinic owns the imaging equipment. Conversely, when the orthopedic surgeon is doing rounds in a facility, claims must be compliantly documented to show only the physician’s professional interpretation (26) of the scan that the hospital technically (TC) performed with its resources.
Failure to apply the appropriate modifier can result in partial reimbursement or denials — contributing to claim delays and cash flow interruptions. As highlighted in 👉 The Cost of Slow EMS Billing: How Delayed Claims Starve Cash Flow, even minor billing workflow disruptions can significantly impact operational stability.
Orthopedic modifier precision directly affects payment timelines.
Drug Wastage and Injection Modifiers
Orthopedic groups administering injectables must properly report drug wastage when applicable. Without correct modifier usage and documentation, payers may refuse reimbursement for the discarded portion.
These underpayments often go unnoticed unless actively tracked — another contributor to margin erosion outlined in 👉 Are Underpayments Eroding Your Practice’s Margins?
Payer-Specific Modifier Requirements
One of the most overlooked risks in orthopedic billing is payer variation.
Each commercial payer — and even Medicare plans — may interpret modifier application differently. Some require documentation upfront. Others deny first and request records later.
Modifier precision alone is not enough if payer enrollment or credentialing gaps exist. As KOVO discusses in 👉Medical Credentialing Services: The Revenue Risk Most Practices Overlook, enrollment inaccuracies can delay reimbursement even when coding is correct.
Revenue protection requires alignment across coding, documentation, and credentialing.
The Most Common Modifier Mistakes in Orthopedic Practices
Even experienced internal billing teams encounter recurring modifier errors:
- Missing RT/LT anatomical distinctions
- Incorrect modifier 50 reporting
- Improper assistant or co-surgeon designation
- Failure to append modifiers for separate reimbursement
- Incorrect modifier sequencing
Each mistake increases denial risk and administrative workload.
When these denials escalate into payment disputes, practices must move beyond basic resubmissions. Structured recovery processes — such as those discussed in 👉 Independent Dispute Resolution (IDR): The Revenue Recovery Tool Most Anesthesia Groups Aren’t Using — demonstrate how specialty practices can recover revenue when payers underpay or dispute claims.
Orthopedic groups facing repeated modifier-related underpayments require similar strategic escalation support.
How Modifier Errors Trigger Denials, Audits, and Underpayments
Modifier errors don’t just cause denials — they create broader financial and compliance risks.
They may lead to:
- Automatic payer edits
- Downcoding and reduced payment
- Increased medical record requests
- Delayed accounts receivable cycles
- Audit exposure when documentation does not align
When these errors are not proactively managed, they contribute to the systemic revenue leakage KOVO addresses across its specialty RCM strategies.
Protecting Orthopedic Revenue with Specialized Modifier Expertise
Orthopedic revenue cycle management requires more than general billing support. It demands:
- Specialty-trained coders familiar with surgical workflows
- Continuous payer policy monitoring
- Proactive documentation validation
- Transparent denial reporting
- Strategic underpayment recovery
👉 Visit our dedicated Orthopedic Medical Billing page.
At KOVO RCM, modifier accuracy is treated as a financial priority — not an administrative afterthought.
Our approach aligns coding precision, credentialing integrity, and denial prevention strategies to reduce the revenue risks outlined across our specialty-focused insights — from credentialing exposure to underpayment recovery and dispute resolution.
Orthopedic groups that treat modifiers strategically — rather than administratively — protect reimbursement, reduce denials, and strengthen long-term financial performance.
🔗More References:
- American Medical Association — CPT® Modifier Definitions & Guidelines
- CMS — Medicare National Correct Coding Initiative (NCCI) Edits
- American Academy of Orthopaedic Surgeons — Coding Resources
- AAPC — Denial Management Best Practices
- CMS — Medicare Claims Processing Manual (Includes Modifier Rules)
- Medicare Appeals & Reimbursement Dispute Overview
- Kovo RCM Blog